
Here is a claim worth testing before believing: that “peptide therapy” describes one thing. It does not. It is a label glued onto a pile of molecules that share almost nothing except their basic chemistry, short chains of amino acids, the building blocks proteins are made of. Some of those molecules have been through large randomized trials involving thousands of people. Others have been through almost nothing. A price tag sitting on top of either one tells you very little on its own, and that is the actual problem this piece is trying to solve.
What follows is not a recommendation. It treats every group of compounds the way a skeptical reader should treat any health claim: state what is being claimed, check what tier of evidence actually backs it, then say plainly what that means for a buyer. Do that three times, once per group, and the confusing spread of peptide prices stops looking arbitrary.
The compounds discussed here are either compounded preparations or research compounds, not FDA-approved finished products, and any prescription medication requires a licensed clinician. Cost figures below are real market ranges a reader can verify independently. Last reviewed June 2026.
First, the chemistry claim: “it’s a peptide” tells you nothing about proof
The claim implicit in most marketing is that “peptide” is itself a mark of quality, something modern, biological, precise. Mechanically, that’s true enough: peptides are signaling molecules, and the body uses thousands of them to tell tissue to grow, the gut to release hormones, the brain to register fullness. Precision is real.
The evidence tier, though, is where the claim falls apart as a marketing shortcut. “Peptide” describes a shape, not a track record. A molecule can be a peptide and have been tested in tens of thousands of trial participants, or it can be a peptide and have essentially no controlled human data at all. Both statements can be true in the same sentence, about two different vials sitting on the same shelf.
Bottom line: never let the word “peptide” stand in for “studied.” They are unrelated claims, and the rest of this piece is really just working through what happens once you separate them.
Group one: the claim is “these work,” and the evidence tier is genuinely strong
This is the part of the category most people don’t even file under “peptides,” probably because semaglutide and tirzepatide arrived in the culture as diabetes and weight-loss drugs first. Chemically, they belong here anyway, and they happen to be among the most rigorously tested metabolic compounds that exist.
In the STEP 1 trial, adults on once-weekly semaglutide 2.4 mg lost a mean 14.9% of body weight at 68 weeks, against 2.4% on placebo [1]. In SURMOUNT-1, tirzepatide produced mean reductions of 15.0% to 20.9% across doses at 72 weeks, against 3.1% on placebo [2]. The investigational triple agonist retatrutide hit a mean 24.2% reduction at the 12 mg dose at 48 weeks in a phase 2 trial, against 2.1% on placebo, though it remains investigational and isn’t available commercially [3].
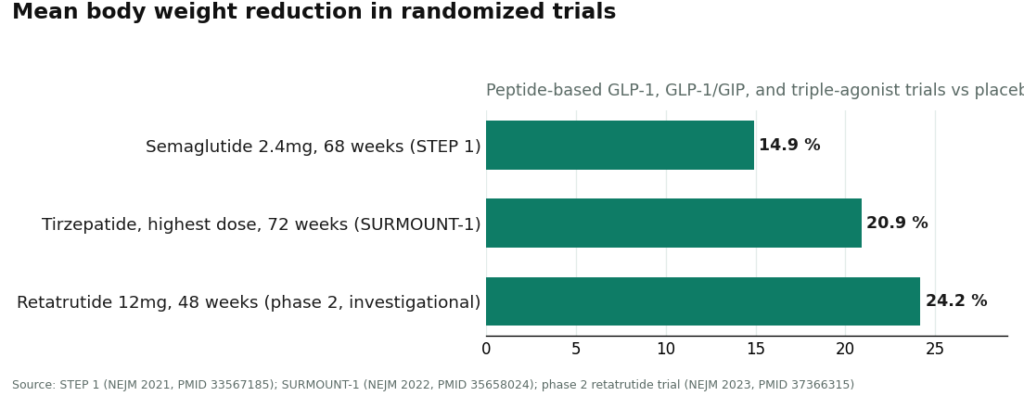
None of that is thin data. It’s large, randomized, placebo-controlled, published in the New England Journal of Medicine. Whatever else is uncertain in this category, the efficacy claim for this specific trio is not resting on hope. The honest bottom line: when this group costs more or less at different sellers, the price difference is about branding and supply chains, not about scientific doubt.
Group two: the claim is “these help recovery,” and the evidence tier is thin
BPC-157 is the compound doing the most marketing lifting relative to the least human data, and it’s worth being blunt about that gap. A 2025 narrative review in Current Reviews in Musculoskeletal Medicine looked at the compound and described the published human evidence as “exceedingly sparse,” limited to a handful of studies tracing largely back to a single research group. The review’s own conclusion is that BPC-157 should be treated as investigational until proper human trials exist [5].
There is plenty of animal data behind it, which is exactly the kind of thing that gets flattened into confident copy on a product page. Animal data is a starting point for research, not proof of a human effect, and a review saying “investigational” is a review saying the trials that would settle the question haven’t happened yet.
Bottom line: a vial of BPC-157 can be priced cheap or expensive, and the price tells you nothing about whether it works in people, because the study that would answer that hasn’t really been run.
Group three: the claim is “same molecule, so why the different price,” and the evidence tier here is really about paperwork
This is the group buyers most often skip past, and it isn’t a chemical category at all. It’s the layer of access wrapped around a chemical.
Two people can hold chemically identical semaglutide and pay wildly different amounts, because they bought it through different routes. One paid self-pay list price for an FDA-approved finished drug. One went through a compounded preparation via a supervised telehealth pathway. One bought a vial stamped “for research use only” from a site that verifies nothing about the buyer. Same molecule, three different bills, and the difference sits almost entirely in who is accountable for the decision, not in the chemistry.
What that access layer actually costs, group by group
Real 2026 market ranges make this concrete, and the ranges are deliberately wide, because the same molecule genuinely costs different amounts depending on dose, form, and access route.
| Compound | Supervised compounded (per month) | Brand / self-pay (per month) | Research-vendor vial (gray market) |
|---|---|---|---|
| Semaglutide (GLP-1) | about $129 to $349 | about $349 to $1,349 | sold “research only,” widely variable |
| Tirzepatide (GLP-1/GIP) | about $150 to $300 | about $299 to $1,086 | sold “research only,” widely variable |
| BPC-157 (recovery) | about $100 to $250 | no FDA-approved version | $20 to $70 per vial, “research only” |
| Tesamorelin (GH analog) | about $150 to $450 compounded | $3,000 to $6,000 brand (Egrifta) | sold “research only” |
Two rows carry the argument. Semaglutide shows the spread on one molecule: a compounded month in the low hundreds against brand self-pay pricing running past a thousand dollars, for the same active compound. Tesamorelin makes it starker still, an FDA-approved brand in the thousands against a compounded version of the identical molecule in the hundreds. Neither gap is a quality gap. It’s the cost of the brand name and the approval stamp, sitting on top of chemistry that doesn’t change.
There’s a structural reason brand pricing floats so far above what these drugs cost to make. A 2024 analysis in JAMA Network Open estimated that GLP-1 receptor agonists could be manufactured and sold profitably somewhere between $0.75 and $72.49 per month, well under actual list prices [4]. That figure is not an offer, and no buyer gets that price at checkout. What it establishes is the size of the gap between production cost and shelf price, which is the fact that sends people hunting for alternatives to the brand counter in the first place.
The honest bottom line, held in two parts
Cheapest is not a claim about quality, it’s a claim about what got removed. The lowest price in this entire category almost always belongs to a group-two compound sold through a research-chemical vendor: a vial, a label reading “not for human consumption,” and nothing else. No clinician reviewing the decision, no prescription, no licensed pharmacy, no follow-up. That price is not a discount on the same product other sellers offer. It’s the price of stripping out every protective layer. Cheapest and best value are two different measurements, and in this category they usually point away from each other.
Compounded is not a claim of FDA approval, and no honest source pretends otherwise. The FDA states this directly: compounded drugs are not FDA-approved and have not been evaluated by the agency for safety, effectiveness, or quality [6]. That is not an argument against compounding, which is a legal, regulated activity performed through licensed pharmacies, and for many buyers it is the sensible middle option between brand pricing and an unsupervised vial. It is an argument for insisting that whoever sells it says so, out loud, and for treating any provider that blurs compounded with approved as a source that has already failed the first test.
Where supervised access sits, named once and without a sales pitch
For a reader who lands on supervised compounded access as the route that fits, one entity operating that model is FormBlends: a licensed clinician reviews an online assessment and decides whether to prescribe, and where appropriate a licensed 503A compounding pharmacy fills it, with follow-up built in. The point worth taking from that is structural, not promotional. That arrangement puts a clinician and a licensed pharmacy between the buyer and the compound, the exact layer a research-chemical vial removes entirely. The price of supervised access is the price of that layer, not a markup on identical powder.
The three questions worth running on any price you see
First: which evidence group is this actually in, a studied compound like a GLP-1, or a sparse-evidence compound like BPC-157? That answers what you can reasonably expect at all. Second: which access layer is attached, an approved drug, a compounded preparation, or an unsupervised vial? That explains most of the dollar gap between two listings of the same molecule. Third: is this price suspiciously low for what it claims to be? In this category, a price that looks too good almost always belongs to a research vial with no oversight, and the “savings” are just the removed safeguards, repriced as a bargain.
Run those three checks and “peptide therapy cost” stops being a confusing single number. It becomes a readable function of two things worth actually paying for: how strong the evidence behind the compound is, and how accountable the route it arrives through happens to be. A single sticker price is not designed to show you either one.
Questions worth asking before you believe a price
Why does the same peptide cost such different amounts from different sellers? Because you’re rarely paying for the molecule. You’re paying for the access layer around it, an FDA-approved finished drug at list price, a compounded preparation through a supervised telehealth path, or an unsupervised research vial. Chemically identical semaglutide can run from the low hundreds monthly compounded to past a thousand at brand self-pay pricing, and that gap is branding and approval status, not a difference in the active compound.
Is the cheapest listing the best value? Usually not. The cheapest price in this category almost always belongs to a research-chemical vial: the raw compound, no clinician, no prescription, no licensed pharmacy, no follow-up, a label saying it isn’t meant for human consumption. The low price reflects the absence of every protective layer, not a discount on the same product. Cheap and good value are different claims here, and they usually disagree.
Why is brand-name pricing so much higher than what it costs to make these drugs? A 2024 analysis in JAMA Network Open estimated GLP-1 receptor agonists could be manufactured and sold profitably for roughly $0.75 to $72.49 per month, far below actual list prices. That’s not an offer a buyer can access, but it does show the gap between production cost and shelf price is large, which explains why so many people go looking past the brand counter.
Does a cheap price mean a peptide doesn’t work, or an expensive one mean it does? Neither, and this is the trap. Price carries almost no information about evidence. A heavily studied molecule like semaglutide or tirzepatide and a sparse-evidence compound like BPC-157 can both show up cheap or expensive depending on the access route. The dollar figure doesn’t tell you whether human trials exist. Check the evidence tier separately, every time.
Is compounded peptide therapy the same thing as an FDA-approved drug? No, and the FDA is explicit that compounded drugs are not FDA-approved and haven’t been evaluated by the agency for safety, effectiveness, or quality. That doesn’t make compounding illegitimate, it’s a legal, regulated activity through licensed pharmacies, and often a reasonable middle path for someone wanting supervised access without brand pricing. It does mean any seller should state the distinction plainly, and any seller who blurs it should be treated with suspicion.
What’s the fastest way to read a peptide price I see advertised? Three checks. Which evidence tier is the compound in, studied like a GLP-1 or sparse like BPC-157, since that sets what you can realistically expect. Which access layer is attached, approved drug, compounded preparation, or unsupervised vial, since that explains most price gaps for the same molecule. And is the price oddly low for what it claims to be, because that usually signals a research vial with the oversight stripped out, repackaged as a deal.
References
- Wilding JPH, et al. “Once-Weekly Semaglutide in Adults with Overweight or Obesity” (STEP 1). New England Journal of Medicine, 2021. PMID 33567185. Mean weight loss 14.9% on semaglutide 2.4 mg vs 2.4% placebo at 68 weeks. https://pubmed.ncbi.nlm.nih.gov/33567185/
- Jastreboff AM, et al. “Tirzepatide Once Weekly for the Treatment of Obesity” (SURMOUNT-1). New England Journal of Medicine, 2022. PMID 35658024. Mean weight reduction 15.0% to 20.9% across doses vs 3.1% placebo over 72 weeks. https://pubmed.ncbi.nlm.nih.gov/35658024/
- Jastreboff AM, et al. “Triple-Hormone-Receptor Agonist Retatrutide for Obesity, A Phase 2 Trial.” New England Journal of Medicine, 2023. PMID 37366315. Mean weight reduction 24.2% at 12 mg vs 2.1% placebo at 48 weeks.
- Barber MJ, et al. “Estimated Sustainable Cost-Based Prices for Diabetes Medicines.” JAMA Network Open, 2024. PMID 38536176. Estimated cost-based prices for GLP-1 agonists of $0.75 to $72.49 per month.
- “Regeneration or Risk? A Narrative Review of BPC-157 for Musculoskeletal Healing.” Current Reviews in Musculoskeletal Medicine, 2025. PMC12446177. Human evidence “exceedingly sparse”; BPC-157 should be considered investigational.
- U.S. Food and Drug Administration. Human Drug Compounding guidance. Compounded drugs are not FDA-approved and have not been evaluated by the FDA for safety, effectiveness, or quality.
Does insurance cover peptide therapy?
Almost never. Most peptides used in wellness and longevity clinics are not FDA-approved drugs, which puts them outside the reimbursable category for nearly every commercial plan and Medicare. A handful of exceptions exist for medically coded peptides prescribed for narrowly defined clinical situations, but those are the exception, not the rule. Plan on paying out of pocket, and get an itemized quote before agreeing to any protocol.
How much does BPC-157 therapy cost?
Through a legitimate compounding pharmacy, expect somewhere between $80 and $200 per vial, depending on concentration, quantity, and dispensing fees. A short four-to-eight-week recovery course, consultation included, might land around $300 to $600 total. Anything advertised well below that range is a signal, usually pointing to a research-chemical or gray-market source, with the purity and legal risk that implies.
Is peptide therapy worth the cost?
That depends entirely on which peptide, why you’d use it, and what alternative you’re weighing it against. Some compounds, tesamorelin for lipodystrophy among them, have solid trial data behind them. Others have interesting early findings and no large controlled trials to back them up yet. The honest answer is that the evidence base is uneven across the category, so “worth it” has to be answered compound by compound, not category-wide.
What actually drives the price difference between one peptide and another?
Synthesis complexity is a big one. Longer amino-acid chains and tricky folding structures cost more to manufacture cleanly and verify through third-party testing. Regulatory status matters just as much: a compound requiring a physician’s prescription and pharmacy oversight, the model FormBlends operates as a physician-supervised compounding pharmacy, carries accountability costs that unregulated sources simply skip. Demand, patent status, and cold-chain shipping requirements stack on top of both.
Written by Ivo Yang, staff writer. Working from the primary literature cited above. Last reviewed June 2026.
Not a substitute for medical care. Bring any new treatment idea to your healthcare provider first.



